Can Emerging Markets Emerge Fast Enough?
The IMS Institute’s annual report on global drug spending predicts a slight rebound in developed markets, despite historically low growth rates. In emerging markets, growth continues to be robust, but is it enough to balance the ongoing stagnancy in Europe and the US?
The IMS Institute’s annual report on global drug spending predicts a slight rebound in developed markets, despite historically low growth rates. In emerging markets, growth continues to be robust, but is it enough to balance the ongoing stagnancy in Europe and the US?

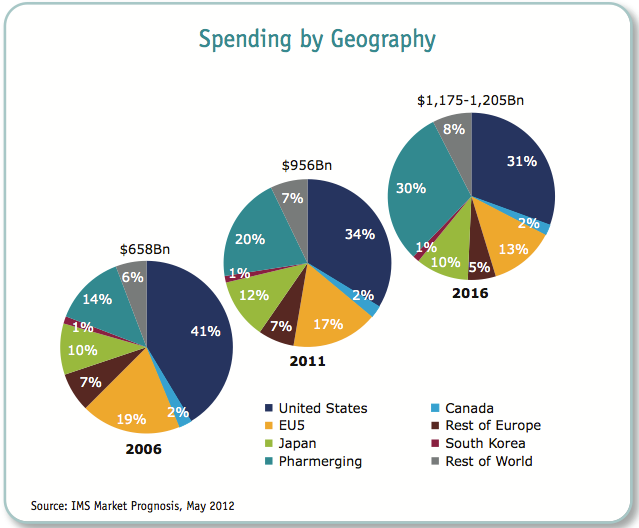

In 2016, the US will spend roughly $892 per person on pharmaceuticals, more than any other country in the world. By contrast, India will spend around $33 per person, according to the IMS Institute’s estimate. But the population of India is nearly four times larger than the US population, which helps account for the fact that countries designated as “pharmerging” markets by IMS, i.e., countries whose citizens earn less than an average of $25,000 a year, per capita, will represent 30% of all drug spending globally, up from 20% in 2011. Developed markets, on the other hand, will backpedal, from 66% of global drug spend in 2011 to an estimated 57% in 2016, according to the IMS Institute’s annual outlook, released today.
Despite drastically divergent levels of income, government outlays and access to medicines in general, the so-called pharmerging markets will be the principle growth drivers over the next five years, due in large part to a spate of government policies intended to bring poor populations into health systems for the first time. Regarding access to medicines, being poor in Mexico is not the same as being poor in India, where even some basic medicines are largely purchased entirely out of pocket by patients.
In Mexico, for example, there’s a basic level of health care provided for low income populations, and in China, 339 million people – a population larger than the entire US population – are expected to enter new government clinics and hospitals in rural areas, said Michael Kleinrock, director of research development at the IMS Institute, on a call with reporters. “These people are getting access to basic medicines, antibiotics, pain killers, medicines for heart disease and even for cancer,” as a direct result of government investment. But there’s a strong incentive for governments to focus on generics, to keep costs down; generics, OTCs and other non-branded products will account for roughly 83 percent of the pharmerging market drug spending increase, the report found. Even so, pharmerging markets will nearly double their cumulative drug spend by 2016; IMS predicts that pharmerging markets will spend upwards of $165 billion on medicines by 2016.
South Korea recently crossed the $25,000 average per capita income, and duly graduated from pharmerging to emerged, noted Kleinrock on the call. South Korea’s crossing of the $25,000 threshold can be witnessed “not just with the living standards in the country, but also all the Korean cars everyone seems to be driving these days,” said Kleinrock.
South Korea aside, several pharmerging countries can boast a growing middle class, even though “countries like Pakistan, Indonesia, India, China and Brazil still have basically 50% or more of their population today living on less than $5,000 a year,” said Kleinrock. The $5,000 mark is significant, since the “typical [average] cost of the most common chronic medicines that people can get in these markets is about $12 a month,” Kleinrock said. “If you’re making $5,000 a year, that’s about one or two percent of your income. Most people in the world are much more comfortable when they’re spending that very low percentage on out of pocket costs for medicines,” as opposed to spending $12 a month on a $500 annual income, for example. When income rises above $5,000, people “can afford to visit a doctor, and they may be diagnosed,” said Kleinrock, adding that there’s “a great deal of discussion” around the emergence of a globetrotting “western disease profile” attributed to outsourced office work from developed countries, and the pustular rise of fast food restaurants and western-style dining.
Does pharma’s strategy for capacity building and industrial policy in certain pharmerging markets include a secretive McDonald’s tie-in? Let’s hope not. On the positive side, IMS reports that 2012 will have been the worst year for patent expiry fall-out in the US, and so a “rebound” is expected to reverberate throughout the developed markets over the next five years. Growth rates will remain at historic lows and are likely to stay that way, but new molecular entities are on the rise, with innovative therapies for Alzheimer’s, autoimmune disease and many other diseases potentially rolling out by 2016. Pricing in developed markets (particularly in the UK and Germany) isn’t likely to improve, with the exception of Japan, which instituted reforms in 2010 that better encourage the adoption of new medicines. Still, drug spending in Japan will only grow slightly, from 1-4%. Japan will lose its number two position in overall drug spending by 2016, with China hopping into the slot, IMS predicts. Brazil will climb up the spending latter as well, bypassing Germany and France to become the fourth largest spender, behind the US, China and Japan, respectively, according to IMS.
For more information on drug spending through 2016, including top therapeutic areas for growth, biosimilar expectations and more, the IMS report, titled The Global Use of Medicines: Outlook Through 2016 is available for free, here.












Addressing Disparities in Psoriasis Trials: Takeda's Strategies for Inclusivity in Clinical Research
April 14th 2025LaShell Robinson, Head of Global Feasibility and Trial Equity at Takeda, speaks about the company's strategies to engage patients in underrepresented populations in its phase III psoriasis trials.


Beyond the Prescription: Pharma's Role in Digital Health Conversations
April 1st 2025Join us for an insightful conversation with Jennifer Harakal, Head of Regulatory Affairs at Canopy Life Sciences, as we unpack the evolving intersection of social media and healthcare decisions. Discover how pharmaceutical companies can navigate regulatory challenges while meaningfully engaging with consumers in digital spaces. Jennifer shares expert strategies for responsible marketing, working with influencers, and creating educational content that bridges the gap between patients and healthcare providers. A must-listen for pharma marketers looking to build trust and compliance in today's social media landscape.


FDA Approves Nipocalimab for the Treatment of Generalized Myasthenia Gravis
April 30th 2025Approval is based on results from the pivotal Vivacity-MG3 trial in which IMAAVY (nipocalimab-aahu) demonstrated superior disease control throughout 24 weeks when compared to placebo plus standard of care.

